|
Articular pathologies and Surgery of the Hand |
|
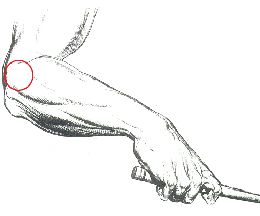
1. Epicondylitis (elbow of the tennis player)
If you want to know more about this topic, book an appointment with the prof. Panfili
|
|
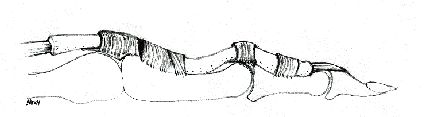
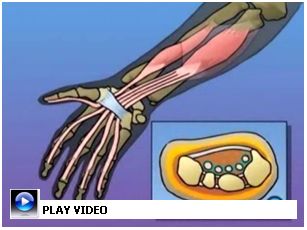
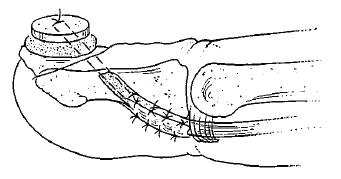
2. The “flick” finger
In case a portion of the tendini is thickened
for an inflammatory process, these slides inside with hard work of
the channel and, sometimes, “they jam”, jamming to level of the
beginning of the same channel. The sliding of the tendini initially
happens exactly to hard work provoking pain and crackle feeling or
can be verified the classic “release” (sees figure b). With the
flesso-extension of the fingers this “difficult” passage repeats
migliaia of times in the course of the day creating the bases of the
chronic inflammation that triggers the progressive already
ingrossati increase of volume of the tendini, creating therefore a
vicious circle that perpetual the inflammatory process.
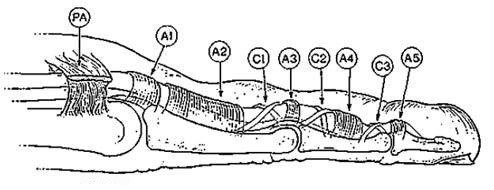
Fig. To: Normal anatomy of the digital channel them with the tendini flessori, the sinoviale membrane and the pulegge.
Affected people l
“finger to release” appears most times spontaneously, without
appearing cause. Sometimes it can be secondary to traumi of the hand
or appears in combination to diseases like diabetes, gotta, morbo of
Dupuytren, reumatoide arthritis, the primary arthrosis of the hand.
The hit age more turns out to be between the 40 and 60 years. The
disease can hit also the children in the first months of life,
usually to level of the 1° metatarso of the inch that remains
blocked in bending. Symptomatology
The palpazione in the region to palmare can be
talora painful and often it reveals the presence of a nodule that
moves during the movements of the finger. In an advanced stage the
finger can turn out blocked in extension or bending because of a
simple inflammatory process of the sinoviale woven one that it
encircles you stretch some and that it comes called “tenosynovitis”.
In this case sometimes the movement of the finger happens with a
crackle, but without the “true release” and just. The radiografico examination is necessary in order to exclude that they can it are to you bony causes to the “block” of the sliding of the tendini. A ecografico examination can reveal in is made begins them the simple tenosynovitis.
Therapy
In it makes begins them some of these remedies can find a justification but in it makes advances, when the episodes of “block” take place every morning and also during the day and the painful symptomatology the surgical treatment becomes ingravescente.
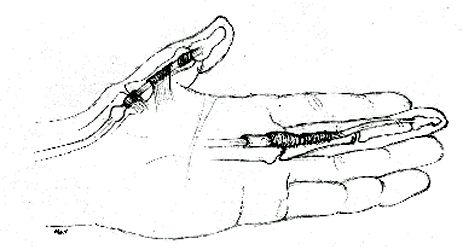
Surgical treatment
The most effective E' and concurs than to
resolve the problem immediately avoiding the progressive damage of
the tendini. The treatment consists in the sbrigliamento of tendini
through the recording of the prossimale portion of the digital
channel them, practically of 1° the pulley (Fig. c). The
participation is amazingly express and hard little minuteren, come
executed in local anesthesia and the patient can immediately move
the fingers after the participation. Sometimes can become necessary
for some days uses it of one metallic stick in order to recover the
complete extension of the finger.
If you want to know more about this topic, book an appointment with the prof. Panfili
|
|
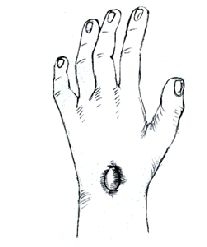
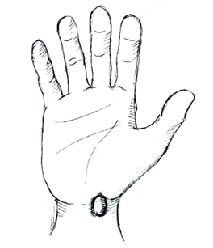
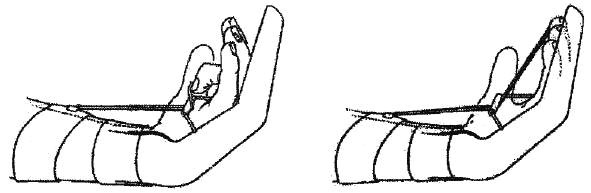
3. The cysts of the wrist
The cysts of the wrist or “sinoviale ganglion”, are neoformazioni much common to dorsal level dell and to palmare of the wrist (see figures).
The gangliari cysts originate with a thin one peduncolo from the deep articulations of the wrist (Fig. c). The cause that determines the appearance of the cysts is today disowned.
Symptomatology Initially to their appearance the cysts can be painful, in order then subsequently to become asymptomatic at rest, generating eventual pain only in occasion of an intense and protratto use of the hand. The volume of the gangliari cysts can vary in the time and for reasons it probably connects you to the metabolism and to the feeding in fact they can talora regrediire completely for recidivare later on.
Diagnosis Essentially clinical the diagnosis I found myself on the center and the morphologic characteristics and of consistency of the neoformazione. The surgeon of the hand can think opportune to advise a radiografico examination of the wrist and the hand in order to evidence eventual concomitant problematic osteo-articular. Sometimes, a ecografico examination in the smaller cysts or the cysts not still obvious can be thought clinical necessary (cysts hidden) but suspected on the base of one painful symptomatology to level of the wrist.
Therapy
In failure case it must take in consideration the surgical treatment.
Surgical treatment
executed in general or plessica anesthesia (peripheral
anesthesia to the base of the limb) and it usually demands a shelter
of a day. The participation resolves to do to completely remove the
cysts with its peduncolo. This can demand sometimes the removal of
one portion of the cap to articulate of the wrist. In such case it
can become necessary, after the participation, I use it of one
polsiera armed to carry for approximately two weeks. If you want to know more about this topic, book an appointment with the prof. Panfili
|
|
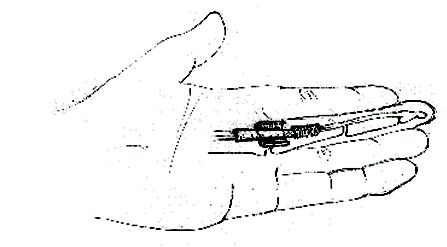
4. The tenosynovitis of De Quervain
In red dark, you stretch of it short
drafter clearly, in red its muscle.
Causes It hits persons who execute repetitive violent movements or much with the wrist or in subjects defedati from the nutrizionale point of view. For this he is frequent in the musicians, in the getlteman given over to the sewing and the embroidery, in who it uses a lot mouse or the keyboard of the computer and in the mothers, species in the last period of breast-feeding, when to raise the child it represents an intense and impegnativo effort. In effects, to the age of De Quervain, this it was known like the disease of the nannies and the ricamatrici.
Discreet possibility exists one to prevent the
appearance of the disease, as an example avoiding to carry out for
hours and hours the same type of movement, using correct positions
and distributing the job, when possible, on the two hands. Symptomatology
Diagnosis
The diagnosis is based on the description of the
symptoms, that they are much characteristic.
An echography can be useful, while the x-ray is useless, since not extension some alteration.
Therapy incruenta In it is made begins them the treatment it is conservativo and it consists in the temporary suspension of the responsible manual activities of the mechanical stimulus to level of the channel.
Which arnica and echinacea and/or non-steroidei (FANS or Cox-2) to a fisioterapia cycle can also come employ natural anti-inflammatory drugs in combination to you.
Fisiokinesiterapia, exacta to the tekarterapia, to try even if often sortiscono do not turn out hope to you to you. E' possible moreover to practice an infiltration of cortisone directly in the channel of the tendini inflames to you. The treatments conserved list to you to you resolve the painful symptomatology in 70% of the patients.
Surgical therapy of the advance shapes
Qaundo the pain is intense and/or persistent or if it
disturbs do not resolve with drugs and the tutor, it becomes
indicated the surgical treatment.
The participation, that it comes carried out with the
anesthesia of all the limb and in Day Hospital, has one duration of
approximately 15 minuteren.
The operation consists in opening the tendinea girdle
that is narrow, therefore to eliminate the friction between girdle
and tendini.
After the participation the hand and the inch come
immobilize in one chalk stick or rigid untutore to you for 10-12
days. Passed this time they come removes the points to you and a
short program of riabilitazione of the hand is begun.
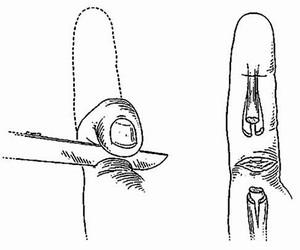
In the photo, the line of cutaneous recording of the
surgical participation
If you want to know more about this topic, book an appointment with the prof. Panfili
|
|
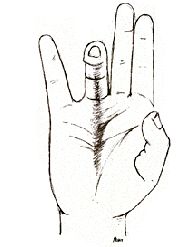
5. Dupuytren disease
The disease of Dupuytren consists in a thickening of wraps to palmare, that is of the interposed woven one between cute of the palm of the hand and the tendini flessori. Such thickening can give origin to a true and own stiff rope from the palm of the hand until to the fingers whom the movement of extension of a finger limits or more fingers rendering impossible the complete opening of the hand (Figure To)
Hit subjects more from pathology Patients of male sex. The disease usually rebels to the age of 40 years and often famous one familiar distribution. Some patients can introduce stricter shapes and in such case the age of insorgence is more premature and the localization diffused to both the hands and more very rarely to the feet.
Symptomatology
The disease rebels much slow and progressive and
manifest with the appearance of one small tumefazione d hard-elastic
consistency that stretches to become a small nodule fibrous or,
sometimes, of an area of cutaneous retraction in the palm of the
hand. Such formations appear of usual in correspondence of the
palmari pliche along the axis of 4° or 5° the finger. Sure patients instead report only begin them sense of rigidity-annoyance localized in the palm of the hand with the compulsiva tendency of massaggiare the cute to palmare, to this clinical phase follow at a distance of time usual, the progressive appearance of the nodule and/or the cutaneous retraction. With passing of the time it is possible to find the formation of true and just a stiff fibrous cord to caorda of arc between the palm of the hand and the finger or the hit fingers. The patient moreover notices of the disease when she states that the palm of the hand cannot completely be supported to plate on one surface like that one of a table (figure B).
Such clinical picture can remain invariato for years and practically to arrest itself definitively or to get exausted itself momentarily for evolvere then progressively until the complete retraction of one or more fingers in the palm of the hand. In the serious cases the retraction of the fingers in the palm of the hand can interfere with the normal daily activities like washing the hands or the ace, wearing gloves or to thread the hands in the pockets.
Therapy
Needle aided microsurgery treatment Draft of one technical minium-invasive, consists in the multiple section of the aponeurotica sclerosis, thickened and retratta, executed with a agosonda based on following is made:
This technique is, unfortunately, a lot often forgotten or not known from the specialists, for which too many sick ones they cannot benefit some.
Classic surgical treatment
The treatment is surgical and consists in the removal of wraps to palmare and digital retratta them. The treatment comes executed in general or pelvic anesthesia (peripheral anesthesia to the base of the limb) and usually demands a shelter of a day. The isolated presence of a nodule does not constitute an indication to the participation, but it demands a periodic control from part of a Surgeon of the Hand. The distribution of the cutaneous manifestations can turn out useful to such care to mark on a representing design the palm of the hands begins them of the disease (Figure C).
If you want to know more about this topic, book an appointment with the prof. Panfili
|
|
6. Syndrome of the Carpal Tunnel
The Carpal Tunnel Syndrome is a disease caused from the jam of the median nerve, that Carpale Tunnel inside crosses the wrist of a called channel. This nerve controls the sensibility of the inch, the index, the mean and of a part of the ring finger and the movements it correlates you to the sinergica activity of small muscles, it calls tenari muscles to you, it situates you to the base of the inch (figure To).
The Carpale tunnel is one circumscribed anatomical region and very defined of the base of the palm of the hand and circumscribed on three sides from boneses of carpo and on the fourth side from a legamento a lot often called Legamento Trasverso of the Carpo. The median nerve with to nine tendini flessori slides in this channel (Figure B).
Causes The Syndrome of the carpale Tunnel is the result of the conflict works them that every time can be verified that produces an increase of pressure inside of the such channel to disturb to the element more weak person than this system, that is the median nerve. Most times the increase of pressure inside of the channel verification for an increase of volume of the membrane that covers the tendini flessori, called condition tenosynovitis, articular luxations, fractures of the wrist that can moreover determine one excessive pressure and a venetuale narrowing from the outside of the responsible channel in its turn of an ulterior increase of the present pressorio regimen inside of the same channel.
Hit subjects more The syndrome of the Carpale Tunnel is one disease much frequent one. Working activities that involve repetitive movements of the fingers and the wrist can inside be the cause of the inflammation of the tendini flessori of the channel and therefore of the suffering of the median nerve. The persons who often work to the PC complain such symptoms and in such cases it is useful to resort to of the ortesi works them.
The women come frequently hit during the pregnancy because of the retention of liquids that inside determines an increase of volume of the channel. The symptoms often are resolved spontaneously with the term of the pregnancy. The women often come hit also in the period of the menopause. The appearance of the characteristic symptoms of the syndrome of the carpale Tunnel often happens in concomitanza with a gessato apparatus applied for one wrist fracture. Diabetic patients or dializza you or with diseases of the tiroide or reumatoide arthritis they can develop a Syndrome of the Carpale Tunnel, often caused just from a thickening of the membrane that covers the tendini flessori.
Symptomatology Formicolio of usual, more emphasized than night the much risvegliare patient and to force it to search one position of the wrist and the hand in order to reduce the annoyance. In the stages more it advances the loss to you of sensibility and the pain appears by day also in concomitanza with simple daily activities like guiding the automobile or reading a newspaper or to hold the cornetta of the telephone or in concomitanza with working activities that demand repeated movements of prensione; Feeling of bruciore (or pain) to the first 3-4 fingers of the hand, often only to 3° and 4° the finger; Often extended pain to the forearm, talora to the arm and more very rarely to the shoulder; REDUCTION DELAL FORCE PRENSILE, with difficulty to seize some objects that can fall without warning from the hands; LOSS OF THE TONE AND MUSCULAR VOLUME; the patients can notice also one “loss” of the musculature to the base of the inch (atrophy tenare). The symptoms can be present in both the hands, but usually they are gets worse on one side.
Diagnosis Beyond that on the base of the clinical history the diagnosis comes mail with the aid of a called examination Elettromiografia (EMG) that concurs the recording of the activity of muscles and the nerves. The examination, of the duration of 15 minuteren approximately, can turn out annoying than more painful generally less (than how much s'immagini) and usually is very tolerated from the patient who immediately after can resume the normal activities (job, guide, sport…). Other nerves can come estimated with the same examination so as to to be sure that the symptomatology reported from the patient is due only to the jam median nerve to the wrist and that is not instead the consequence of neurological problems it generalizes to you.
The RMN (artroscan) of the wrist is useful, therefore as the RXo of the wrist, especially if osteoarticolari problems to level of the wrist are suspected.
Surgical therapy
The symptomatology is of solvable usual surgical,
however in the stages it begins them and light, it can
incruentemente talora be resolved. The identification and the
medical treatment of the eventual disease of base, the change of
particular a working gestualità, the use of a rigid tutor (polsiera
army, in order to guarantee a correct postura of the wrist in rest
position during the working activity, can be revealed useful in
order to reduce the jam on the median nerve. Endoscopic therapy In cases it selects, we execute with succeeding also the technique to you for via endoscopy, that small recording consists in practicing one on the depositor to palmare de wrist through which comes inside introduced of the carpale tunnel a probe to fiber optics that concurs to visualize the legamento trasverso and, at the same time, sezionar decompressing it the nerve. The duration of the participation is short and comes of usual executed in local anesthesia and regimen of day-hospital therefore that the patient will be able to return to the own room the same day. The patient must begin immediately to move the fingers.
The resumption of manual activities to read like
dressing themselves, eating and the personal hygiene happen within
one week from the participation. I use suit of the operated hand happens in the 4-6 turn weeks. The surgical treatment determines of usual the immediate passing of the formicolio nocturnal. It can residuare, however, for some weeks or, sometimes, also for months a dolenza localized to level of the scar to palmare that it can appear reddened and hardened. Such it disturbs are assigns to you however to resolve itself spontaneously also at a distance of a year. In the serious cases, when the jam of the nerve lasts from much time, the surgical treatment can not resolve the symptomatology completely.
Contenitiva Polsiera
The use of one polsiera armed also with night can,
sometimes, resolve the formicolio that it disturbs the sleep.
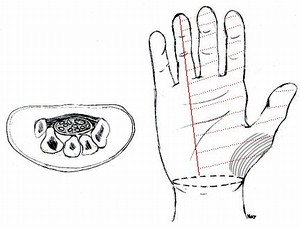
Medical Tetapia Also medical therapy (FANS or Cox-2 and Gabapentin) antiinflammatory somministrata for oral way or an infiltration of cortisone directly in the carpale Tunnel can, sometimes, resolve the symptomatology. If the symptomatology does not improve the surgical treatment it turns out necessary and it has the scope to create more space in the carpale Tunnel being reduced therefore the jam on the nerve. The treatment consists in one small recording of the cute of the palm of the hand and in the successive recording of the legamento trasverso of carpo (Figure C).
If you want to know more about this topic, book an appointment with the prof. Panfili
|
|
7. Lesions of the flexor tendinis
The muscles that flettono or close the fingers are found to level of the forearm and flessori muscles are called. Such muscles are in a position to flettere the fingers thanks to cordiformi structures calls tendini that they become part to the falangi. The inch possesses along flessore muscle that through along you stretch some becomes part to the falange tos be distant them. The other fingers have two flessori muscles ognuna, the superficial flessore muscle and deep the flessore muscle. You stretch some of the superficial flessore muscle one becomes part to the falange intermediate and she has the task to fold the finger to level of 2° the articulation of every finger, while that one of the deep flessore becomes part to the falange tos be distant them and has the task to fold also 3° the articulation of every finger. To level of the fingers the tendini they passes in a digital channel that it turns out constituted deeply from a sinoviale membrane that encircles both the tendini and of it it favors the mutual sliding and more superficialally from ciamati fibrous thickenings pulegge of reflection cha they have the task to maintain the tendini to contact with the bony plan during the bending of the falangi.
A deep cut to level of the wrist, the palm or the fingers can interest tendini flessori and also the important nervous and vascular structures. The lesion can appear practically initially simple but to be much complex. When ransom, you stretch some it is behaved as elastic and a two extremity goes away one from the other. Since the greater part of the lesions from cut happens while the fingers are flesse, the cut tendinee extremities goes away ulteriorly when the finger comes straightened for the clinical examination. To second of the center of the lesion we can have the section of a solo you stretch some and the finger can partially maintain the ability to flettersi. If the lesion happens more neighbor to the base of the finger can have the section of both the tendini and the finger completely loses the ability to flettersi. At last the lesion from cut puo sezionare only partially you stretch some and the finger can maintain the ability subsequently to flettersi but to lose it for one secondary breach.
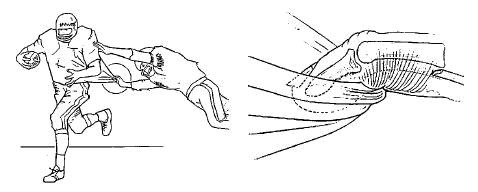
For all these reasons are not unfortunately infrequent that a tendinea lesion comes or not riconosciuita or underrated when the examination of the wound from cut comes made in hurried and inadequate way. We at last remember the subcutaneous breaches from tendinea avulsion to level of its insertion tos be distant them that they are involved often sure disciplines sport like rugby or the climb, lesions that ill-fatedly pass initially inossevate. The interested finger more is the ring finger. The lesivo mechanism consists in a forced extension while the flessore muscle strongly is contracted sometimes and that determines the avulsion of stretches of it and its retraction also to level of the palm. Also such lesion goes ready recognized because you stretch some must be recovered and be made to slide through the intact digital channel them within at least 7-10 days. Beyond such period you stretch some degenerates and swell and it will not be more possible to make it to slide in its channel and reinserir it in the bone.
The tendinea relief
The tendini they are constituted from alive cells and
woven connecting. If the tendinee extremities are brought back to
contact taking part surgical, the guarigione has beginning inside of
stretches of it thanks to the cellular member and outside of you
stretch of it thanks to the connettivale member. The recovery of the
tendinee extremities is not however always simple. Often it must
record a part of the digital channel them with the relative ones
pulegge, woven that they come been involved to they time in the
repair process.
The other complicanza is instead the yielding of
sutura or tendinea repair, and also in this case that happens if the
riabilitativo outline equally is not corrected. Practically in post
operating and based on the type of lesion and executed repair the
area center of the lesion it will come or protect from every
movement or will come granted a particular outline riabilitativo. Ta
l and outline concur with the finger or the fingers center of the
lesion an active movement in extension and liabilities in bending so
that a sliding of the tendini happens without some resistance to
level of sutura tendinea in order at least 4-6 weeks.
After which it will come granted to the patient to
begin weak people active movements in bending without resistance
reminding that the complete process of guarigione usually demands
approximately 3 months. In the greater part of the cases a complete
recovery of the movement will not be had however also because the
cicatriziale adhesion is from considering a part of the normal
process of tendinea guarigione.
And' important to emphasize that through controls clinicians it only draws near the terapista or the same surgeon to you will be in a position to understanding if the patient is executing the riabilitazione correctly. In the inveterate tendinee lesions dealt not correctly or recognized sometimes the cicatriziale process is not such that it becomes necessary to clean up the sliding channel completely and to replace you stretch some or both the tendini with a tendineo graft captured from the same hand or others you leave of the body. Also in this case the patient will be subordinate to a particular riabilitativo outline.
If you want to know more about this topic, book an appointment with the prof. Panfili
|
|
8. The arthrosis of the hand
Which thing is? Most frequent between the diseases of the articulations it is sure the Arthrosis, disease characterized from the slow and progressive degeneration of the cartilage to articulate. The hand comes hit from the arthrosis in some characteristic centers that are, in frequency order, the interfalangee articulations tos be distant them, the prossimali interfalangee articulations and the articulation trapeze-metacarpale, to the base of the inch. Very rarely they come hit the metacarpofalangee articulations or the wrists.
From what it is caused? It comes defined commonly osteoartrosi primary because of usual the cause is not characterized any. Sometimes it comes defined secondary because he turns out consequent or to traumi or working activity characterized from repeated gestures or to articular infections. The arthrosis can be manifested moreover associate to other reumatiche, often confused diseases with the osteoartrosi primary, like as an example the psoriasica arthropathy or the reumatoide arthritis. The arthrosis of the hand progresses with the age of the patient. Signs radiograph to us typical of the arthrosis of the hands can be found in 8O% of the population beyond the 65 years of age; to of under of the 45 years it appears with equal frequency in the male and feminine sex while beyond 5O the years they mainly turn out hit the women.
Symptoms The light symptoms appear gradually and are of usual and not correlabili to the signs it radiographs to us characterizes to you from the narrowing of the space to articulate and from the formation of osteofiti or bony appuntimenti. Only 1O% of the population introduce symptoms like pain, rigidity to articulate and loss of function of such intensity to demand the participation of the doctor.
Treatment The conservativo treatment, beyond to the occasional somministrazione of anti-inflammatory (FANS or Cox-2), can comprise cortico infiltrations steroids, cycles of fisioterapia like paraffin baths, ultraplays or ionoforesi and I use it of position tutors to carry above all during is made acute of the inflammation. In rare cases and for particular clinical manifestations the surgical participation only becomes necessary.
Particular pictures
The osteoartrosi erosive consist in acute inflammatory varying of the osteoartrosi primary and also hit of usual the women in menopause being able to begin also in 3° and 4° the decade. In this case the articulations more hit, also in asymmetric way, are the interfalangee to be distant them of the fingers. The debut can be also much painful to level of one single articulation. The osteoartrosi erosive, with the exception of the osteoartrosi primary, determine one fast and massive destruction of the cartilage to articulate and the bone provoking, in the arc of some years, marked axial shunting lines. The base of the last one falange of the fingers appears of increased usual and dancing causing one clean limitation of the prensione. Also in the osteoartrosi erosive the treatment in is made begins them is sintomatico and consists in the use of small digital tutors them in is made acute of the inflammation. When the instability picture to articulate limits the total function of the single hand the surgical treatment, based of usual on the artrodesi or “fusion” of the articulations hit, it can be a useful treatment.
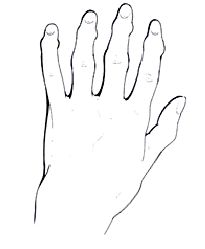
The nodules of Eberden are painful rigonfiamenti situate to you on the dorsal face of the interfalangee articulations to be distant them of the fingers. They are the sign more obvious than arthrosis of the hand and they are manifested more frequently approximately 1O times in the woman who in the man. These nodules are developed initially in way graduate them, without pain and of usual they only hit a finger for time. To the fine all the fingers can introduce the nodules of Eberden and confer to the hand a homogenous knotted aspect (Fig. 1).
Very rarely the development of the nodules turns out more express with reddening and pain in particular after extended use of the hand. Sometimes the manifestations and the symptoms are therefore acute to simulate an infection. Of usual after some months the flush and the tumefazione, recedono spontaneously, leaving to of over of the dorsal face of these small articulations one thickened and not painful callosity. The rigonfiamento to articulate turns out caused from a thickening of the soft woven ones beyond that from one proliferation of cartilage to level of the bony insertion of the cap, the legamenti and the tendini. This progressive increase of the articulation can succeed in to determine a lateral shunting line or in bending of the falange they tos be distant. Very rarely a surgical treatment is indicated. Only the in a marked manner turned aside painful articulations and justify the surgical treatment that consists in the artrodesi that is the “fusion” to articulate that it restores the necessary stability to one good taken.
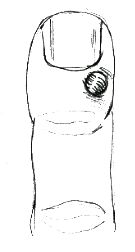
The cysts mucosae or mucoidi are generally associated formations to the arthrosis of the small articulations to be distant them of the fingers or the inch. They are small peduncolate cysts that contain sinoviale liquid and the articulation and the base of the nail are developed between. One thinks that these cysts always are associated to dorsal osteofita.
The cysts turn out of hard consistency to the
palpazione and because of their progressive increase of volume the
cute that it covers to them can become much thin one, nearly
transparent. Left in center can determine a dystrophy of the nail
that is of usual one of the causes that push the patient from the
doctor. An other problem consists in the fact that cute that it
covers the cysts can become more and more thin with the risk to
ulcerarsi determining an infection of the articulation. Of cysts in
the event mucoide in evolution, above all if much painful one, the
surgical treatment of escissione of the cysts with its peduncolo and
the osteofita small is sure the ideal treatment.
If you want to know more about this topic, book an appointment with the prof. Panfili
|
|
|
 <
TO
<
TO
 <
B
<
B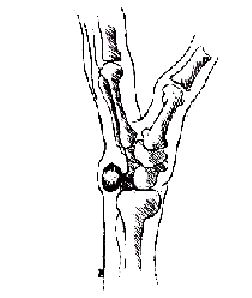 <
C
<
C

 To
To
 B
B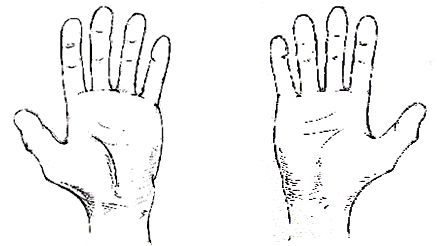 C
C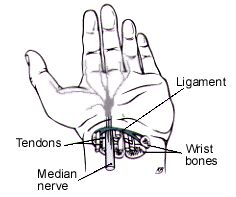 To
To
 B
B C
C
 < Nodules of Eberden
< Nodules of Eberden
 < Cysts mucosae
< Cysts mucosae