Articular pathologies and Surgery of the Foot
Hallux valgus
The foot is constituted from 26 boneses and very 33 articulations. The boneses of the foot are disposed in three groups that, proceeding from the leg, compose the skeleton of the footstep (the posterior part of the foot), of metatarso (the part center them of the foot) and the fingers or falangi (the part more to be distant them). The foot represents lofty capolavoro a biomeccanico one that expresses the adaptation of the man to the atmosphere who encircles it and in particular to the ground on which it walks and to the footwear.
The foot is born before the shoe and as such it would have to deserve some care in more… and instead it comes maltrattato and forced, especially from the feminine sex, in splendid and elegant footwear, that they end in order to damage, talora irrimediabilmente the fingers and particular the first finger: the alluce.
The alluce I am worth is a deformity of 1° the finger of the foot and in particular of the metatarso, the long bone that precedes the falangi, that is the boneses that form the skeleton of the fingers of the feet. The appearance of the disturbance is subdola, because it is characterized from an intense pain, that it can be attenuated in order then to ripresentarsi later on, while the deformity of the manifest finger in one phase only advanced of the disease.
Symptomatology
The alluce I am worth initially announces under shape of one small surrounding inflamed shelf the epifisi (head) of the 1° metatarso, above all after a extended friction against tomaia of the shoe triggering the famous bursitis.
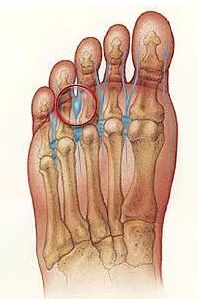
The alluce it comes defined I am worth, because it is become deformed towards the outside and with the tip turned towards the other fingers, that it triggers like consequence the deformation of the 1° metatarso, that becomes sporgente in its turn and launches, that is deformed towards the inside. In particular, it is spoken about alluce I am worth when the angle between first and the second metatarso, correspondents exactly to the first one and to according to finger, are advanced to 8°. This is valued with one simple made x-ray to execute with the sottocarico foot.
Generally, at the beginnig of the disturbance the pain has had is to the inflammation of the woven ones that they cover the shelf and that they are found under of it like also the sublussazione of the articulation of the first finger, like consequence of the shunting line.
The new position of the articulation forces the person to walk in way scorretta, with the risk to assume positions mistaken in the attempt not to feel the pain. Occupying space in the shoes, moreover, the bony shelf imposes the use of comfortable footwear, if not quite manufactured on measure, in order to avoid that the other fingers overlap from each other. In more, all the risente vertebral column of the new situation. The speed with which the disturbance it gets worse depends on the natural predisposition, the type of life that is lead and on the shoes that are worn.
|
Alluce I am worth light |
Alluce I am worth mean |
Alluce I am worth serious |



|
Preoperative x-ray |
Post-operative x-ray |


|
Post-surgical shoe |
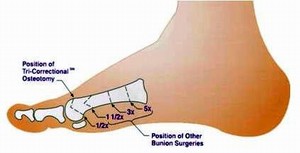
Center of the osteotomies in order to correct the alluce I am worth |


Before the
participation After the participation
Causes
Alluce I am worth congenital
when the metatarsale head, (last part of the metatarso that it is articulated with the base of the falange) is round or can record very other factors:
-
Relatives: for es. the so-called foot egizio (the alluce it is longer of the other fingers)
-
Anatomical (legacies to the same anatomy of the foot)
Alluce I am worth acquired
The root cause of a alluce I am worth acquired is tied to the use of footwear scomode, like shoes to tightened tip with high heels, because they provoke an excessive pressure on the fingers, than ago to move is the alluce is the mignolo towards the inner part of the foot, in this way, the other fingers turn out crushed. These pressures still increase more when the shoes have the high heel, because all the weight of the body is moved automatically towards the front part of the foot. Also the use of rigid shoes much can prevent the natural bending of the fingers when it is walked, because the musculature of the foot is weakened, facilitating the appearance of alterations.
NB: More of 90% of the persons hit are women, even with a “foot egizio”.
Prevention
-
ATTENTION to the shoes that are used since been able to provoke damages and disturbs irreversible;
-
PODOLOGO: to o from a good podologo, helps senz' better other to living;
-
TO USE COMFORTABLE SHOES: tomaia in soft skin and with the tip of the cappellotto wide, with a heel that does not exceed i 4 cm.
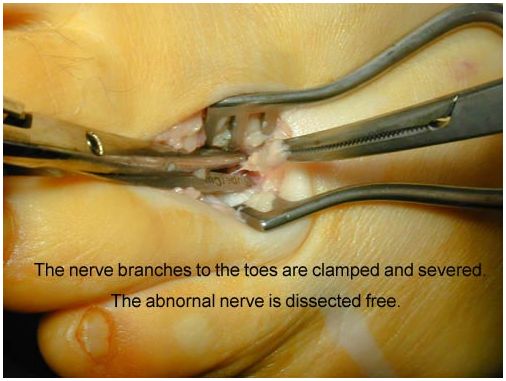
Microsurgery therapy
They are more than the 100 surgical techniques used in order to correct the alluce I am worth, that ago very to comprise that this deformity does not represent only an aesthetic uneasiness, but a disturbance works them frequent and painful that hits the women above all. All the orthopaedic ones support with justice that the alluce I am worth is from only operating if provokes pain and however if the quality of life pregiudica in some way characterizes them and not only for an aesthetic defect.
After the participation that is carried out in native place-regional anesthesia and regimen of Day Hospital the patient will have to avoid to load to earth for the first 24 hours (the stampelle with norm is not necessary). The pain is only a memory thanks to the modern ortomolecolari and anestesiologiche techniques of preparation and post participation that renders the surgery a more serene and decidedly calm event.
Until the end of the third month after the participation it is advised to avoid the elevations on the tip of the feet; to guide with the automatic machine is possible already after 10-12 gg if the participation has been carried out on a single limb, otherwise is preferred to attend after the first month; to adhere itself to the post-operative radiological controls and to all which will come indicated subsequently.
If you want to know more about this topic, book an appointment with the prof. Panfili